Lungs: CBSE Class 11 NCERT Notes
Cheatsheet Content
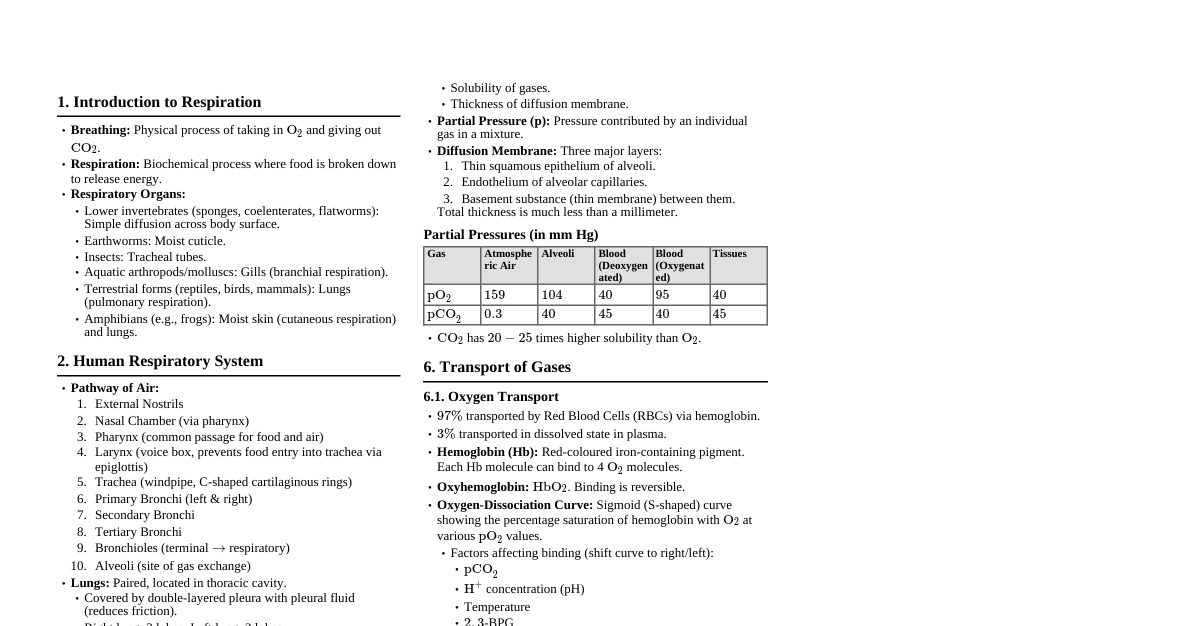
1. Respiratory Organs Humans have a pair of external nostrils opening out above the upper lips. The nasal chamber opens into the pharynx , a common passage for food and air. The pharynx opens through the larynx region into the trachea . Larynx (sound box): Cartilaginous box which helps in sound production. During swallowing, epiglottis (a thin elastic cartilaginous flap) covers the glottis (opening of the larynx) to prevent food entry into the larynx. Trachea: Straight tube extending up to the mid-thoracic cavity, dividing at the 5th thoracic vertebra into right and left primary bronchi . Each bronchus undergoes repeated divisions to form secondary and tertiary bronchi and bronchioles , ending up in very thin, irregular-walled vascularised bag-like structures called alveoli . The branching network of bronchi, bronchioles, and alveoli comprises the lungs . Humans have two lungs, enclosed in a double-layered pleura , with pleural fluid between the layers, reducing friction on the lung surface. The outer pleural membrane is in close contact with the thoracic wall, while the inner pleural membrane is in contact with the lung surface. The part starting with the external nostrils up to the terminal bronchioles constitutes the conducting part (transports air to the alveoli, clears it from foreign particles, humidifies and brings it to body temperature). The alveoli and their ducts form the respiratory or exchange part (site of actual diffusion of $O_2$ and $CO_2$ between blood and atmospheric air). Lungs are situated in the thoracic chamber , which is anatomically an air-tight chamber. The thoracic chamber is formed dorsally by the vertebral column, ventrally by the sternum, laterally by the ribs, and on the lower side by the dome-shaped diaphragm . The anatomical setup of lungs in the thorax is such that any change in the volume of the thoracic cavity will be reflected in the lung volume. This arrangement is essential for breathing. Respiration involves: Breathing or pulmonary ventilation (atmospheric air drawn in, $CO_2$-rich alveolar air released out). Diffusion of gases ($O_2$ and $CO_2$) across alveolar membrane. Transport of gases by blood. Diffusion of $O_2$ and $CO_2$ between blood and tissues. Utilisation of $O_2$ by cells for catabolic reactions and resultant release of $CO_2$ (cellular respiration). 2. Mechanism of Breathing Breathing involves inspiration (inhalation) and expiration (exhalation). Movement of air into and out of the lungs is carried out by creating a pressure gradient between the lungs and the atmosphere. Inspiration: Occurs when pressure within lungs (intra-pulmonary pressure) is less than atmospheric pressure. Contraction of diaphragm (flattens) increases volume of thoracic chamber in antero-posterior axis. Contraction of external intercostal muscles lifts ribs and sternum, increasing volume of thoracic chamber in dorso-ventral axis. Overall increase in thoracic volume leads to increase in pulmonary volume. Increase in pulmonary volume decreases intra-pulmonary pressure to less than atmospheric pressure. Air rushes into the lungs. Expiration: Occurs when intra-pulmonary pressure is higher than atmospheric pressure. Relaxation of diaphragm and intercostal muscles. Diaphragm returns to its dome-shaped position; sternum and ribs return to normal position. Decreases thoracic volume, which decreases pulmonary volume. Decreases pulmonary volume increases intra-pulmonary pressure above atmospheric pressure. Air is expelled from the lungs. Forced inspiration/expiration involves additional muscles (e.g., abdominal muscles, internal intercostals). A healthy human breathes 12-16 times/minute . Spirometer: Instrument to measure respiratory volumes and capacities. 3. Respiratory Volumes and Capacities Tidal Volume (TV): Volume of air inspired or expired during a normal respiration. Approx. 500 mL . ($6000-8000$ mL/min). Inspiratory Reserve Volume (IRV): Additional volume of air a person can inspire by a forcible inspiration. Approx. 2500-3000 mL . Expiratory Reserve Volume (ERV): Additional volume of air a person can forcibly expire. Approx. 1000-1100 mL . Residual Volume (RV): Volume of air remaining in the lungs even after a forcible expiration. Approx. 1100-1200 mL . Inspiratory Capacity (IC): Total volume of air a person can inspire after a normal expiration. $IC = TV + IRV$. Expiratory Capacity (EC): Total volume of air a person can expire after a normal inspiration. $EC = TV + ERV$. Functional Residual Capacity (FRC): Volume of air remaining in the lungs after a normal expiration. $FRC = ERV + RV$. Vital Capacity (VC): Maximum volume of air a person can breathe in after a forced expiration OR maximum volume of air a person can breathe out after a forced inspiration. $VC = ERV + TV + IRV$. Total Lung Capacity (TLC): Total volume of air accommodated in the lungs at the end of a forced inspiration. $TLC = RV + ERV + TV + IRV$ or $TLC = VC + RV$. 4. Exchange of Gases Occurs at alveoli and between blood and tissues . Primarily by diffusion , dependent on pressure/concentration gradient , solubility of gases, and thickness of membranes. Partial pressure ($P_{O_2}, P_{CO_2}$): Pressure contributed by an individual gas in a mixture of gases. Partial pressures (in mm Hg): Respiratory Gas Atmospheric Air Alveoli Blood (Deoxygenated) Blood (Oxygenated) Tissues $P_{O_2}$ 159 104 40 95 40 $P_{CO_2}$ 0.3 40 45 40 45 Diffusion Membrane: Three major layers: Thin squamous epithelium of alveoli. Endothelium of alveolar capillaries. Basement substance (thin basement membrane) between them. Total thickness is much less than a millimeter. $P_{O_2}$ in alveoli (104 mmHg) > $P_{O_2}$ in deoxygenated blood (40 mmHg) $\implies$ $O_2$ diffuses from alveoli to blood. $P_{CO_2}$ in deoxygenated blood (45 mmHg) > $P_{CO_2}$ in alveoli (40 mmHg) $\implies$ $CO_2$ diffuses from blood to alveoli. $P_{O_2}$ in oxygenated blood (95 mmHg) > $P_{O_2}$ in tissues (40 mmHg) $\implies$ $O_2$ diffuses from blood to tissues. $P_{CO_2}$ in tissues (45 mmHg) > $P_{CO_2}$ in oxygenated blood (40 mmHg) $\implies$ $CO_2$ diffuses from tissues to blood. Solubility: $CO_2$ is 20-25 times more soluble than $O_2$. This means $CO_2$ can diffuse through the diffusion membrane much faster per unit pressure difference. 5. Transport of Gases 5.1 Oxygen Transport 97% of $O_2$ is transported by red blood cells (RBCs) . 3% of $O_2$ is carried in dissolved state by plasma . Hemoglobin (Hb): Red coloured iron-containing pigment in the RBCs. $O_2$ binds with Hb to form oxyhemoglobin ($HbO_2$). $Hb + 4O_2 \rightleftharpoons Hb(O_2)_4$ Each Hb molecule can carry a maximum of four molecules of $O_2$. Binding of $O_2$ with Hb is primarily related to partial pressure of $O_2$ ($P_{O_2}$) . Other factors: $P_{CO_2}$, $H^+$ concentration, temperature. Oxygen-Dissociation Curve: Sigmoid curve obtained when percentage saturation of Hb with $O_2$ is plotted against $P_{O_2}$. In the alveoli (high $P_{O_2}$, low $P_{CO_2}$, less $H^+$ concentration, lower temperature), factors favour the formation of oxyhemoglobin. In the tissues (low $P_{O_2}$, high $P_{CO_2}$, high $H^+$ concentration, higher temperature), factors favour the dissociation of $O_2$ from oxyhemoglobin. Every 100 mL of oxygenated blood delivers around 5 mL of $O_2$ to the tissues under normal physiological conditions. 5.2 Carbon Dioxide Transport 20-25% of $CO_2$ is transported by RBCs as carbaminohemoglobin ($HbCO_2$). 70% of $CO_2$ is transported as bicarbonate ions ($HCO_3^-$). 7% of $CO_2$ is carried in dissolved state through plasma . Binding of $CO_2$ to Hb is related to $P_{CO_2}$. $P_{O_2}$ is a major factor affecting this binding. In tissues (high $P_{CO_2}$), $CO_2$ binds with Hb. $CO_2 + H_2O \xrightarrow{\text{Carbonic Anhydrase}} H_2CO_3 \xrightarrow{} H^+ + HCO_3^-$ (This reaction is catalysed by the enzyme carbonic anhydrase , present in high concentration in RBCs and in small amounts in plasma.) $HCO_3^-$ diffuses into the plasma, and to maintain ionic balance, chloride ions ($Cl^-$) move from plasma into RBCs ( chloride shift ). In alveoli (low $P_{CO_2}$, high $P_{O_2}$), $CO_2$ dissociates from carbaminohemoglobin and $HCO_3^-$ converts back to $CO_2$. Every 100 mL of deoxygenated blood delivers approximately 4 mL of $CO_2$ to the alveoli. 6. Regulation of Respiration Specialised centre in the medulla oblongata ( respiratory rhythm centre ) primarily responsible for regulation. Another centre in the pons region ( pneumotaxic centre ) can moderate the functions of the respiratory rhythm centre. Pneumotaxic centre reduces the duration of inspiration, thereby altering the respiratory rate. Chemosensitive area: Adjacent to the rhythm centre, highly sensitive to $CO_2$ and $H^+$ ions. Increase in $CO_2$ or $H^+$ concentration activates this centre, which in turn signals the rhythm centre to make necessary adjustments in the respiratory process for elimination of these substances. Receptors associated with aortic arch and carotid artery also recognise changes in $CO_2$ and $H^+$ concentration and send necessary signals to the rhythm centre. Role of $O_2$ in respiratory regulation is quite insignificant. 7. Disorders of Respiratory System Asthma: Difficulty in breathing causing wheezing due to inflammation of bronchi and bronchioles. Emphysema: Chronic disorder where alveolar walls are damaged, reducing respiratory surface. Major cause is cigarette smoking . Occupational Respiratory Disorders: Caused by exposure to dust in industries (e.g., grinding, stone-breaking). Leads to inflammation and fibrosis (proliferation of fibrous connective tissue). E.g., Silicosis , Asbestosis . Workers should wear protective masks.