Nursing Process & Critical Thinking
Cheatsheet Content
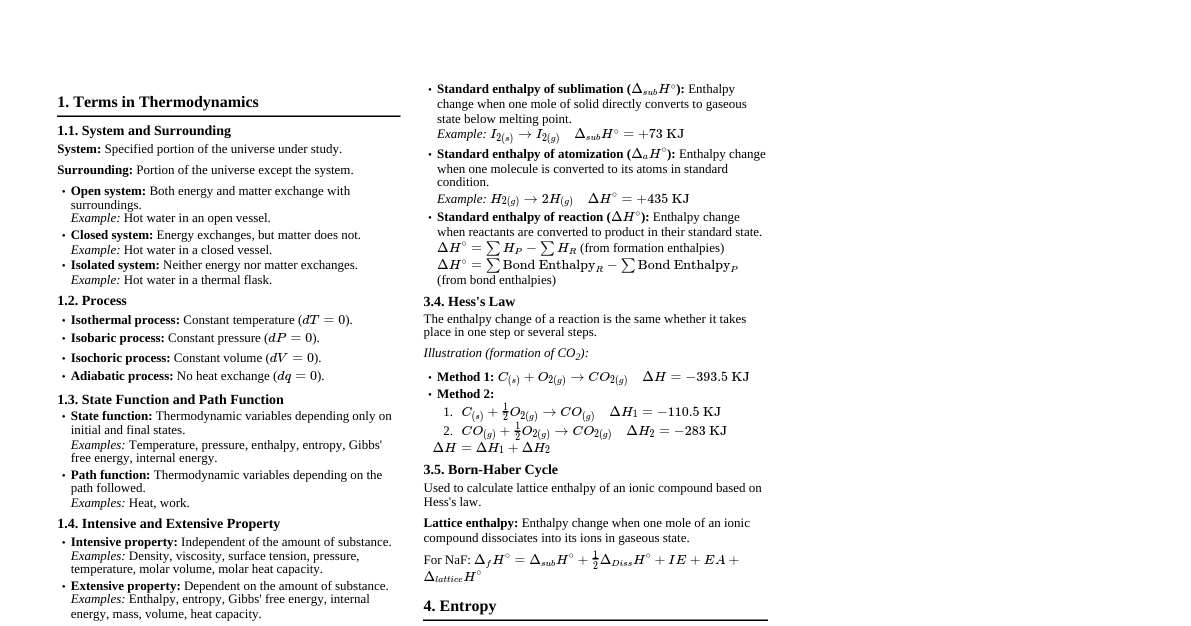
1. Critical Thinking in Nursing Definition: A purposeful, goal-directed way of thinking to make judgments based on evidence. ANA Definition: A purposeful, organized cognitive process supporting clinical decision-making, judgment, and action. Importance in Nursing Process: Key element in Assessment, Diagnosis, Planning, Implementation, Evaluation. Allows nurses to gather/analyze info, identify patterns, make sound decisions, provide high-quality care. Helps identify patient needs, problems, accurate diagnoses, and appropriate care plans. Anticipate problems, adjust care plans. Prioritize, organize, and delegate tasks efficiently. Make ethical decisions, respect patient autonomy. Skills of Critical Thinking: Critical Analysis: Applying questions to determine essential data, discard unnecessary info. Inductive Reasoning: Generalizations from specific observations (e.g., new medication reduces BP in a group, so it might be effective for others). Deductive Reasoning: Specific conclusions from general principles (e.g., patient with diabetes has high blood sugar, so medication dose needs increase). Differentiating Facts & Opinions: Facts: Objective, verifiable through evidence. Opinions: Personal beliefs, subjective, not necessarily evidence-based. Evaluating Accuracy of Information: Assess source credibility. Verify facts with reliable sources. Examine language and tone for objectivity. Recognize biases. Novice vs. Expert Thinking: Novice Thinker Expert Thinker Organizes knowledge as separate facts; relies on resources. Stores knowledge in organized, structured manner; easy recall. Lacks experiential knowledge (e.g., breath sounds). Has storehouse of experiential knowledge (e.g., abnormal breath sounds). Focuses on actions, may forget to assess before acting. Assesses and thinks through before acting. Needs clear-cut rules. Knows when to bend rules. Often unaware of resources. Aware of resources and how to use them. Hindered by anxiety, lack of self-confidence. More self-confident, less anxious, more focused. Relies on step-by-step procedures; focuses on procedure, not patient response. Knows when to skip/combine steps; focuses on both procedure and patient response. Uncomfortable if patient condition precludes exact procedure. Better idea of suspected problems, questions more deeply, collects more relevant data. 2. The Nursing Process Definition: A systematic, patient-centered critical thinking model for clinical reasoning and judgment. ANA Definition: A professional's approach to identifying, diagnosing, and treating human responses to health and illness. Overview: A series of overlapping steps (not linear) to provide individualized, holistic, effective, and efficient care. Purposes: Improve patient outcomes. Provide individualized care. Enhance patient safety. Improve patient satisfaction. Reduce omissions and duplications. Save time and energy. Protect nurses (outlines standard of care). Benefits: Promotes quality care, consistency, collaboration, safety, satisfaction, goal attainment, positive outcomes, efficiency, and professional language. Characteristics: Patient-Centered: Respects individual needs, preferences, values; nurse as advocate. Interpersonal: Basis for therapeutic process between nurse and patient. Collaborative: Functions with inter-professional teams for shared decision-making. Dynamic and Cyclical: Phases interact and influence each other. Requires Critical Thinking: Vital for identifying problems and implementing interventions. 3. Assessment (First Step) Introduction: First step of nursing process; gathering information (physical, psychological, social) through observation, interview, etc. Data Cues: Physical (height, weight, swollen joints). Reported (headache, nausea). Psychological (depression, confusion, anxiety). Social (single-parent, recently bereaved). Laboratory results (low hemoglobin, high blood sugar). Types of Assessment: Initial Nursing Assessment: Within specified time after admission; complete database for problem identification. Problem-Focused Assessment: Determine status of specific problem from earlier assessment (e.g., hourly vital signs for fever). Emergency Assessment: During emergencies to identify life-threatening situations (e.g., rapid airway, breathing, circulation assessment). Time-Lapsed Reassessment: Several months after initial assessment; compares current status with previous data. Collection of Data: Gathering relevant information about patient's health status, physical, psychological, social conditions, and factors affecting health. Includes health history, physical exam, lab results, other personnel input. Types of Data: Subjective Data (Symptoms): From patient's point of view (feelings, perceptions, concerns); obtained via interview; relies on patient's experience. Objective Data (Signs): Measurable data obtained via observation, physical exam, lab tests; can be seen, heard, felt, verified by others. Sources of Data: Primary Source: The client (direct). Secondary Sources: Family, significant others, healthcare professionals, medical records, diagnostic test results (indirect). Methods of Data Collection: Observation: Using senses (looking, listening, touching, smelling) to gather data. Interview: Planned communication with a purpose (e.g., nursing health history). Directive: Highly structured, nurse controls (e.g., emergency). Non-directive (Rapport Building): Client controls, nurse builds rapport. Stages: Opening/Introduction, Body/Development, Closing. Physical Examination: Systematic data collection for objective data. Techniques: Inspection, Palpation, Percussion, Auscultation. Includes History Taking, Head-to-Toe Assessment, Review of Systems. Organization of Data: Data must be organized for usefulness. Agencies use admission assessment formats (written/computerized). Maslow's Hierarchy of Needs: Prioritizes basic needs. Physiological needs (air, food, water, sleep). Safety needs (security, protection). Love and belonging needs (friendship, family). Esteem needs (respect, value, recognition). Self-actualization needs (full potential, personal growth). 4. Validation of Data Definition: "Double-checking" or verifying data for accuracy and factualness. When to Validate: Discrepancies between subjective and objective data. Client's statements vary at different times. Importance: Ensures assessment info is complete. Ensures objective and subjective data agree. Obtains additional info. Differentiates between cues (data) and inferences (nurse's interpretation). 5. Documentation of Data Purpose: Recording and storing collected assessment information. Importance: Accurate documentation is essential for communication among healthcare team. Ensures continuity of care and evaluation of treatment response. Example: "Tea 150 ml, Juice 200 ml, 1 egg" instead of "appetite good". Criteria for Documentation: Use permanent ink, legible writing. Never leave blank lines. Record chronologically. Record date and time with each contact. Document in a timely manner (as close to real-time as possible). Do not chart in advance. Include signature and designation. Use professional language, avoid abbreviations. Only include notes of care provided by you (unless designated recorder in emergency). Do not include bias (document conclusions supported by data). Methods: Paper Charts & Electronic Health Records. Open-ended Methods: Narrative description of observations. Checklist Methods: Summarizes findings, ensures consistency, reduces omissions. Combination Methods: Checklist with space for narrative. Specialty Methods: Abbreviated formats for specific areas (e.g., outpatient surgery). 6. Nursing Diagnosis (Second Step) Introduction: Second step of nursing process; pivotal for care planning and interventions. Definition (NANDA, 1990): A clinical judgment about individual, family, or community responses to actual and potential health problems/life processes. Provides basis for selecting nursing interventions. Types of Nursing Diagnosis: Actual Nursing Diagnosis: Describes a client problem present at assessment, based on signs/symptoms. Example: Fluid volume deficit related to persistent diarrhea and vomiting as evidenced by decreased urine output. Risk Nursing Diagnosis: Problem does not exist, but factors make client vulnerable. Example: Risk for infection related to altered immunologic response. Wellness Nursing Diagnosis: Judgment about motivation, desire, and readiness to enhance well-being. Example: Readiness for enhanced parenting as evidenced by mother expressing a desire to enhance a conducive environment for children’s growth. Syndrome Nursing Diagnosis: Cluster of predicted actual or potential diagnoses to a particular situation. Example: Rape trauma syndrome related to anxiety about potential health problems as manifested by anger, genitourinary discomfort, and sleep pattern disturbance. Example: Risk for disuse syndrome (includes impaired physical mobility, risk for impaired tissue integrity, etc.). Purposes: Identifies nursing priorities. Directs nursing interventions. Provides common language for communication. Guides outcome formulation. Basis for evaluation of care. Helps with staff assignments. Components of Nursing Diagnosis: Problem (Diagnostic Label): Describes client's actual or potential health problem; specific and concise (e.g., Deficit knowledge , Altered body temperature ). NANDA quantifiers: altered, deficient, excessive, ineffective, impaired. Etiology (Related Factors): Probable cause of the problem; helps formulate interventions (e.g., impaired hand coordination , prolonged bed rest ). Joined by "related to (R/T)". Defining Characteristics (Signs & Symptoms): Cluster of signs/symptoms indicating the diagnostic label. For actual diagnoses, these are patient's signs/symptoms; for risk diagnoses, none are present. Joined by "as manifested by". Example: Impaired skin integrity related to decreased blood circulation and immobility as manifested by damaged tissue, swelling and warmth of the wound and skin around the site of injury is reddish. Diagnostic Process: Uses critical thinking (analysis & synthesis). Analyzing Data: Compare data against standards (identify significant cues). Cluster cues (generate tentative hypotheses). Identify gaps and inconsistencies. Identifying Health Problems, Risks, and Strengths: Determine if problem is nursing, medical, or collaborative. Establish client's strengths, resources, coping abilities. Formulating Diagnostic Statements: Three-part statement (PES format): P (Problem), E (Etiology), S (Signs & Symptoms). Only for actual diagnoses. Example: Impaired skin integrity related to friction and shear from frequent repositioning as manifested by redness and swelling. Two-part statement: Problem + Etiology. Used for risk and actual diagnoses. Example: Risk for fluid volume deficit related to excessive perspiration. One-part statement: Only Problem/Diagnostic Label. Used for wellness and syndrome diagnoses. Example: Readiness for enhanced family coping. Variations in Basic Format: "Unknown etiology" (e.g., Altered body temperature related to unknown etiology ). Splitting etiology components (e.g., risk for impaired skin integrity related to prolong immobility secondary to paralysis of all extremities ). Including "possible" (e.g., Possible low self-esteem related to loss of job ). Adding a second part to problem component (e.g., Knowledge deficit (foot care) related to lack of adequate information ). "Complex factors" in etiologic segment (e.g., Chronic low self-esteem related to complex factors ). Avoiding Errors in Diagnostic Statements: Write client's response, not medical diagnosis. Identify NANDA label, not a symptom. Identify client's response to treatment/test, not test itself. Identify client's response to equipment, not equipment itself. Identify problem, not goal. Avoid legally inadvisable statements. Use professional, not prejudicial, judgment. Avoid circular statements. Use only one problem in diagnostic label. Medical Diagnosis vs. Nursing Diagnosis: Medical Diagnosis Nursing Diagnosis Made by physician. Statement of nursing judgment made by nurses. Etiology focused. Care focused. Nurse's action is dependent. Nurse's action is independent. Oriented to pathology. Oriented to individual. Within scope of medical practice. Within scope of nursing practice. Made only for patients. Made for patients, family members, or caregivers. Specifies illness/condition (alteration of structure/function). Two people may have same disease. Focused on person's physiological/psychological responses to health problems/illness. Two people with same disease may have different responses. Stays same as long as disease is present. May change day to day as human response changes. Example: Myocardial infarction. Example: Activity intolerance related to decreased cardiac output. 7. Planning (Third Step) Introduction: Process of thinking about activities to achieve desired goals, based on foresight. Begins after diagnosis. Definitions: Kozier (1975): Deliberative systematic phase involving decision-making and problem-solving. Potter & Perry (2001): Client-centered goals established, interventions designed to achieve them. Types of Planning: Initial Planning: Initiated ASAP after admission/assessment; establishes database, identifies nursing diagnoses and interventions. Ongoing Planning: Done by all nurses working with patient; occurs at shift beginning; updates plan, facilitates problem resolution, manages risk, promotes function. Discharge Planning: Anticipating and planning for needs after discharge; ensures patient knowledge for self-care. Purposes of Nursing Care Plan: Defines nurse's role. Provides directions for individualized care (roadmap). Coordinates care among healthcare team. Promotes holistic treatment, defines specific goals. Monitors progress, allows adjustments. Directs client care activities. Ensures continuity of care. Processes of Planning: Establishing Priorities: Preferential sequence for addressing diagnoses/interventions. High Priority: Life-threatening (airway, circulation, safety, pain). Medium Priority: Non-emergent, non-life-threatening (e.g., anxiety, imbalanced nutrition). Low Priority: Affects future well-being, long-term needs (e.g., deficient knowledge, self-care deficit). Considerations: Client's beliefs/values, client's priorities, resources, urgency, medical treatment plan. Often uses Maslow's hierarchy of needs. Setting Goals and Expected Outcomes: Goal: Broad statement of desired change (e.g., improve nutritional status ). Time-limited. Expected Outcome: Specific, measurable change in patient's status in response to nursing care (e.g., Gain 5 kg weight by April 25 ). More specific, observable criteria for evaluation. Can be combined: Improved nutritional status as evidenced by weight gain of 5 kg criteria by April 25. Types of Goals: Short-term Goal: Objective behavior/response expected in short time (usually Example: Client will achieve normal body temperature by 4 hrs. Long-term Goal: Objective behavior/response expected over longer period (days, weeks, months). Used for chronic issues, discharge planning. Example: Patient will stop consuming tobacco within 60 days. Components of Goal/Expected Outcomes: Subject: The client or attribute of client (e.g., client's pulse ). Verb: Specifies action client performs (e.g., administer , walk ). Directly observable. Conditions or Modifiers: Circumstances under which behavior is performed (e.g., Walks with the help of cane ). Criterion of Desired Performance: Standard for evaluation (time, accuracy, distance, quality). Example: Weighs 75 kg by April (time) , Lists five out of six signs of diabetes (accuracy) . Guidelines for Writing Goals & Expected Outcomes: Patient-centered: Focus on client responses, not nurse activities. Singular goal or outcome: Each goal/outcome addresses only one behavior/response. Observable: Change in patient status must be observable (physiological, knowledge, perception, behavior). Measurable: Use quantifiable terms; avoid vague qualifiers (normal, acceptable, stable). Time-limited: Indicates when response is expected; realistic time frames. Mutual factors: Patient and nurse agree on direction/time limits. Realistic: Achievable based on assessment, capabilities, limitations, resources. Selecting Nursing Interventions and Writing Nursing Orders: Actions nurses perform to achieve client goals. Focus on eliminating/reducing etiology of diagnosis. If etiology cannot be changed, treat signs/symptoms. For risk diagnoses, focus on reducing risk factors. 8. Implementation (Fourth Step) Introduction: Action-oriented step where interventions are performed to achieve goals. Nursing Interventions: Actions/measures nurses take to promote, maintain, or restore health. Direct Care: Performed through interaction with client. Indirect Care: Performed away from client, on their behalf (e.g., collaboration, environment management). Types of Nursing Interventions: Independent Nursing Interventions (Nurse-Initiated): Actions nurses are licensed to initiate based on skills/knowledge; no physician order needed. Example: Planning mouth care for impaired oral mucous membrane. Dependent Nursing Interventions (Physician-Initiated): Actions requiring an order from physician/other healthcare professional. Example: Administering medication (nurse is responsible for knowledge of drug). Collaborative Interventions: Actions carried out with other health team members (PT, dietician, etc.). Reflects overlapping responsibilities. Example: Informing PT department for crutch walking, coordinating sessions, assisting client. Process of Implementation: Reassessing the Patient: Continuous process; identifies new diagnoses or need to modify care plan. Not evaluation, but gathering info to ensure appropriateness. Reviewing and Revising the Existing Nursing Care Plan: After reassessment, compare data to validate diagnosis and determine intervention appropriateness. Modification Steps: Revise assessment data, revise nursing diagnosis, revise specific interventions, choose evaluation method. Organizing Resources and Care Delivery: Equipment: Ensure availability and working condition. Personnel: Nursing staff work together as needed. Environment: Safe and conducive to therapies; prevent injury (e.g., assist devices, clear pathways). Patient: Ensure physical and psychological comfort (e.g., address nausea, pain). Anticipating and Preventing Complications: Recognize risks from illness/treatment, adapt interventions, evaluate benefits vs. risks, take prevention measures. Implementing Nursing Interventions: Requires cognitive, interpersonal, and psychomotor skills. Cognitive Skills: Application of critical thinking, good judgment, clinical decision-making. Interpersonal Skills: Trusting relationship, caring, clear communication with patient/family; perceptive of verbal/nonverbal cues. Psychomotor Skills: Integration of cognitive and motor activities (e.g., injection requires anatomy knowledge + coordination). Methods of Implementation: Direct Care Method: Activities performed through patient interactions. Activities of Daily Living (ADLs): Ambulation, eating, dressing, bathing, grooming. Instrumental Activities of Daily Living (IADLs): Shopping, meal prep, house cleaning, managing finances, taking meds. Physical Care Techniques: Turning, positioning, nursing procedures, medication administration. Lifesaving Measures: Restore physiological/psychological homeostasis (e.g., emergency meds, CPR, crisis counseling). Counseling: Helps client use problem-solving to manage stress, facilitate relationships (emotional, intellectual, spiritual, psychological support). Teaching: Important responsibility; teach principles, procedures, techniques; assess learning needs; consider cultural/social factors. Controlling for Adverse Reactions: Understand potential side effects of meds/treatments; record reactions, stop, consult physician. Preventive Measures: Promote health, prevent illness. Primary Prevention: Reduce risk factors (health education, immunizations, physical fitness). Secondary Prevention: Early detection and treatment (screening tests: mammograms, Pap smears, colonoscopy). Tertiary Prevention: Minimize effects of chronic illness/disability (rehabilitation, managing diabetes, preventing pressure sores). Indirect Care Method: Activities performed away from patient but on their behalf. Communicating Care Delivery: Document treatment and client's response; clear, concise, to the point. Delegating, Supervising, and Evaluating Work of Other Staff: Coordinate and delegate tasks; nurse assigning tasks is responsible for ensuring completion per standard. 9. Evaluation (Fifth Step) Introduction: Final step; crucial to determine if patient's condition improved after nursing process. Ongoing process. Evaluation of Goal Achievement (Five Components): Collecting data related to desired outcomes. Comparing data with outcomes. Relating nursing activities to outcomes. Drawing conclusions about problem status. Continuing, modifying, or terminating the nursing care plan. Reassessment of Care Plan: If goal met, discontinue that portion of plan. Unmet/partially met goals require continued intervention. Steps: Reassessment, Redefining diagnoses, Goals and expected outcomes, Intervention, Discontinuing a care plan, Modifying a care plan.