Musculoskeletal & Dermatology USMLE Note
Cheatsheet Content
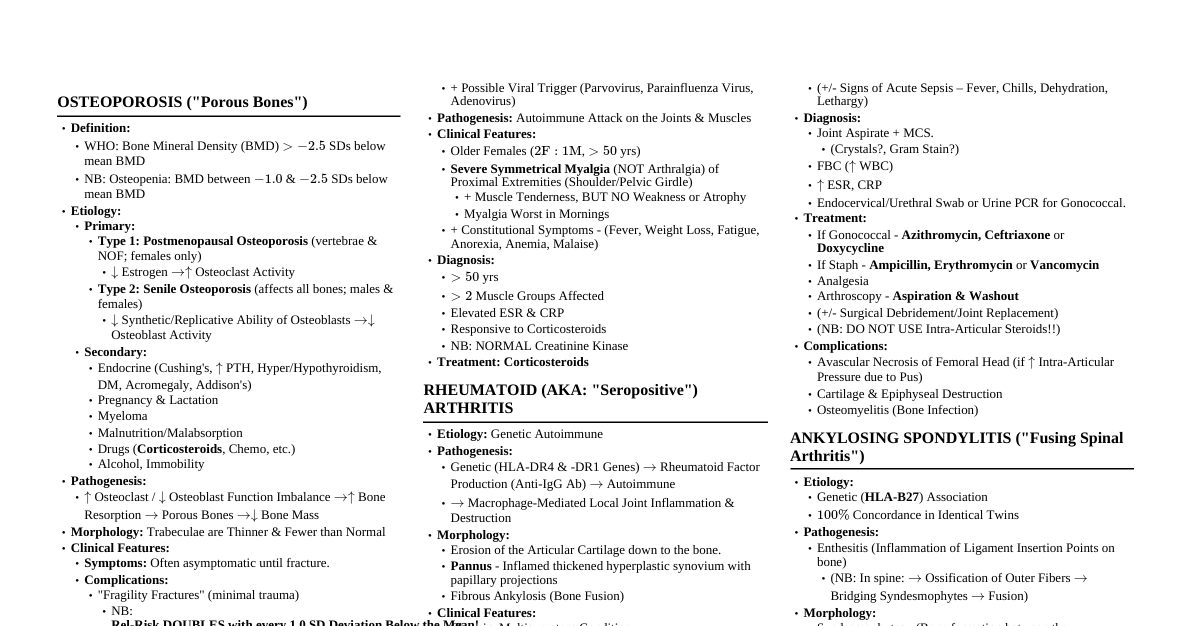
ANATOMY & PHYSIOLOGY - Back & Spinal Cord Lumbar Puncture: Needle enters subarachnoid space (L3/L4 or L4/L5). Horizontal line through iliac crests is L4. Spinal cord ends at L2 (adults), L3 (children). Dural sac extends to S2. Check for increased ICP before procedure (cerebellar tonsil herniation risk). Internal Vertebral Venous Plexus (Epidural Space): Valveless, connects with pelvic/abdominal/thoracic veins. Route for cancer metastasis to vertebrae/cranial cavity. Herniated IV Disc: Most common at L4/L5 or L5/S1 (lumbar), C5/C6 or C6/C7 (cervical). Usually posterolateral (thin posterior longitudinal ligament). Lumbar herniation often involves nerve root one number below (e.g., L4/L5 compresses L5 root). Presents with radicular pain, weakness. Diagnose with straight leg raise test, MRI. Abnormal Spinal Curvatures: Kyphosis: Exaggerated thoracic curvature (e.g., osteoporosis, disk degeneration). Lordosis: Exaggerated lumbar curvature (e.g., pregnancy, spondylolisthesis, potbelly). Scoliosis: Lateral deviation/torsion (e.g., poliomyelitis, leg-length discrepancy). Caudal Regression Syndrome: Agenesis of sacrum/lumbar spine. Associated with poorly controlled maternal diabetes. Flaccid leg paralysis, dorsiflexed foot contractures, urinary incontinence. Spinal Stenosis: Abnormal narrowing of spinal canal (most common in lumbar region), usually >60 years old. Causes: Degenerative arthritis (IV disc shrinkage, facet joint arthritis, hypertrophied ligamentum flavum). Symptoms: Lower extremity pain/numbness/weakness, neurogenic claudication (pain with walking). Pain improves with stooped/flexed position ("shopping cart sign"), worsens with extension. ANATOMY & PHYSIOLOGY - Upper Limb Rotator Cuff Muscles (C5-C6): Supraspinatus, Infraspinatus, Teres Minor, Subscapularis (SITS). Reinforce shoulder joint (except inferiorly). Draw humerus head into glenoid during abduction. Tendonitis: Pain with abduction. Tears: Inability to abduct. Supraspinatus: Most commonly injured (impingement between humeral head & acromion). Assessed by "empty/full can" test. Latissimus Dorsi (C6-C8, Thoracodorsal nerve): Extension, adduction, internal rotation of humerus. Subacromial Bursitis: Often due to calcific supraspinatus tendinitis, painful arc of abduction. Overuse Injuries of Elbow: Medial Epicondylitis (Golfer's Elbow): Repetitive flexion (forehand shots). Lateral Epicondylitis (Tennis Elbow): Repetitive extension (backhand shots). Ulnar Collateral Ligament Injury: Connects medial epicondyle to ulna. Common in throwers (valgus stress). Brachial Plexus Injuries (C5-T1) Nerve Roots Causes of Injury Presentations Axillary Nerve C5-C6 Fractured surgical neck of humerus, anterior dislocation of humerus. Flattened deltoid, loss of arm abduction (>15°), loss of sensation over deltoid/lateral arm. Musculocutaneous Nerve C5-C7 Upper trunk compression. Loss of forearm flexion/supination (Coracobrachialis), loss of sensation over lateral forearm. Radial Nerve C5-T1 Compression of axilla ("Saturday night palsy"), humerus fracture (midshaft/supracondylar), repetitive pronation/supination (supinator canal injury). Triceps weakness (axillary injury), wrist drop (loss of elbow/wrist/finger extension), loss of sensation over posterior arm/forearm/dorsal hand, ↓ grip strength. Supinator canal injury: "finger drop" without wrist drop/sensory deficits. Median Nerve C5-T1 Supracondylar fracture of humerus (proximal), carpal tunnel syndrome, wrist laceration (distal). Proximal: "Pope's blessing" (loss of flexion of lateral fingers, inability to oppose thumb), loss of wrist flexion, thenar eminence atrophy, loss of sensation over thenar eminence and lateral 3½ fingers. Distal: "Ape hand" (thumb adducted, cannot oppose/abduct), thenar atrophy, sensation spared (palmar cutaneous branch). Recurrent Branch of Median Nerve Superficial laceration near flexor retinaculum. Motor innervation to thenar muscles lost (immobilizes thumb), sensation intact. Ulnar Nerve C8-T1 Fracture of medial epicondyle ("funny bone" - proximal), fractured hook of hamate (distal). Loss of finger abduction/adduction (interossei), "ulnar claw" on digit extension (paralysis of medial lumbricals), radial deviation of wrist upon flexion (proximal lesion), loss of wrist flexion/medial finger flexion, loss of sensation over medial 1½ fingers/hypothenar eminence. Ulnar Paradox: Proximal lesions may have less obvious clawing due to loss of flexor digitorum profundus. Long Thoracic Nerve C5-C7 Axillary lymph node dissection, lateral chest wall injury. Scapular winging (serratus anterior paralysis), weakness in abducting arm above horizontal. Common Humerus Fractures & Associated Neurovascular Injuries Surgical neck: Axillary nerve, posterior humeral circumflex artery. Midshaft: Radial nerve, profunda brachii artery (deep brachial artery). Supracondylar: Brachial artery, median nerve. Anterolateral displacement $\rightarrow$ radial nerve injury. Anteromedial displacement $\rightarrow$ median nerve and brachial artery injury. Posterior displacement $\rightarrow$ ulnar nerve injury. Medial epicondyle: Ulnar nerve. Wrist & Hand Fractures/Conditions Distal Radius Fractures: Smith's fracture: Ventral angulation, distal fragment anteriorly displaced (fall on dorsum of flexed wrist). Colles' fracture: Dorsal angulation, distal fragment dorsally displaced ("dinner fork deformity," fall on outstretched hand). Ulnar styloid process avulsion common. Scaphoid Fracture: Most common carpal bone fracture. Cause: Fall on outstretched hand (hyperextended, radially deviated wrist). Presentation: Persistent wrist pain, tenderness in anatomical snuff box. Complication: Avascular necrosis (AVN) and nonunion due to retrograde blood supply. Diagnosis: XR (may take 1-2 weeks), MRI (most sensitive early). Lunate Dislocation: Fall on outstretched hand. "Lonely lunate" sign on lateral XR. May precipitate acute carpal tunnel syndrome (median nerve injury). Metacarpal Neck Fracture ("Boxer's Fracture"): Direct blow with closed fist. Most common in 4th/5th metacarpals. Carpal Tunnel Syndrome: Entrapment of median nerve. Presentation: Paresthesia/pain/numbness in median nerve distribution (first 3 digits, radial half of 4th). Weakness of thumb abduction/opposition. Thenar eminence atrophy (sensation spared). Signs: ⊕ Tinel sign, ⊕ Phalen maneuver. Causes: Pregnancy, RA, hypothyroidism, diabetes, acromegaly, dialysis-related amyloidosis, repetitive use. Treatment: Longitudinal incision through transverse carpal ligament. Cubital Tunnel / Ulnar Tunnel Syndrome: Ulnar nerve compression at elbow (cubital tunnel) or Guyon's canal (wrist). Presentation: Paresthesias over medial 1.5 fingers and ulnar dorsum of hand. Claw hand, weakened grasp/pinch. Exacerbated by flexion (e.g., cell phone use). Guyon's canal: Classically seen in cyclists. Intrinsic Hand Muscles: Thenar (Median nerve): Opponens pollicis, Abductor pollicis brevis, Flexor pollicis brevis (superficial head). Hypothenar (Ulnar nerve): Opponens digiti minimi, Abductor digiti minimi, Flexor digiti minimi brevis. Dorsal Interossei (Ulnar nerve): Abduct fingers. Palmar Interossei (Ulnar nerve): Adduct fingers. Lumbricals (1st/2nd: Median; 3rd/4th: Ulnar): Flex MCP, extend PIP/DIP ("L-shape"). "Clawing": Imbalance of extrinsic flexors/extensors and intrinsic muscles. Distal lesions of median or proximal ulnar nerves. Affected fingers extend at MCP, flex at DIP/PIP. Thoracic Outlet Syndrome (TOS) Compression of blood vessels or nerves in thoracic outlet (between clavicle & 1st rib). Compression of: Lower trunk of brachial plexus ("Klumple's palsy"): Upper extremity numbness, tingling, weakness (worse with arm elevation). Subclavian vein: Upper extremity swelling. Subclavian artery: Exertional arm pain, weak distal pulses. Most common location: Scalene triangle (anterior & middle scalene muscles, 1st rib). Brachial plexus & subclavian artery pass through. Subclavian vein runs anteromedial. Causes: Anomalous cervical rib, 1st rib malunion, scalene muscle hypertrophy/anomalies/injury, Pancoast tumor. Interscalene nerve block: Anesthetizes brachial plexus. Transient ipsilateral diaphragmatic paralysis due to phrenic nerve involvement. ANATOMY & PHYSIOLOGY - Lower Limb Knee Joint Cruciate Ligaments: ACL: Lateral femoral condyle to anterior tibia. Resists anterior tibial movement. PCL: Medial femoral condyle to posterior tibia. Resists posterior tibial movement. Collateral Ligaments: Resist varus/valgus deformity. MCL: Medial epicondyle of femur to medial condyle of tibia. Resists valgus stress. LCL: Medial epicondyle of femur to head of fibula. Resists varus stress. Menisci: Two crescent-shaped fibrocartilaginous pads between tibia & femoral condyles. Appear triangular on MRI. Common Hip & Knee Conditions MCL Injury: Twisting injury or blow to lateral knee (valgus stress). LCL Injury: Rarely isolated, often trauma to medial knee. "Unhappy Triad": Damage to ACL, MCL, and medial meniscus (lateral meniscus injury more common). Acute knee pain, instability. ACL Injury: Sudden decelerations/pivots on extended knee. Excessive anterior tibial motion. Rapid hemarthrosis (middle geniculate artery supply). Bursitis: Trochanteric Bursitis: Inflammation of gluteal tendon/bursa lateral to greater trochanter. Sharp lateral hip/thigh pain, worse with pressure/walking. Prepatellar Bursitis ("Housemaid's knee"): Between patella & skin. Caused by excessive kneeling. Suprapatellar Bursitis: Superior extension of synovial cavity. Common for intraarticular injections. Anserine Bursitis: Pain along medial knee, tenderness 4cm distal to joint margin. Common in obesity/overuse. Baker Cyst: Extrusion of synovial fluid into gastrocnemius-semimembranosus bursa. Popliteal fluid collection. Often asymptomatic, may cause posterior knee pain. Rupture can mimic DVT. Ankle Sprains: Anterior Talofibular Ligament: Most common overall ("Always Tears First"). Due to overinversion/supination. Anterior Inferior Tibiofibular Ligament: Most common high ankle sprain. Femoral Neck Fracture: Associated with osteopenia/osteoporosis. Shortened, externally-rotated leg. Risk of AVN of femoral head (medial circumflex artery compromise). Hip Dislocation: Posterior (90%): Dashboard injury (posterior force on internally rotated, flexed, adducted hip). Limb shortened, flexed, medially rotated. Anterior: Hip in abduction & external rotation. Complications: Sciatic nerve injury, AVN of femoral head. Patella Fracture: Direct impact or excessive force through quadriceps tendon. Acutely swollen knee, patella tenderness, inability to extend knee against gravity, palpable gap in extensor mechanism. Lower Extremity Nerves Nerve Roots Causes of Injury Presentations Femoral Nerve L2-L4 Pelvic fracture, retroperitoneal hematoma (anterior to iliopsoas), saphenous vein stripping. ↓ Thigh flexion, leg extension (difficulty with stairs). Loss of sensation over anterior/medial thigh and medial leg. Absent patellar reflex. Sciatic Nerve L4-S3 Herniated disc, piriformis syndrome, posterior hip dislocation, injections into inferomedial/inferolateral buttock. Weakness of all muscles below knee. Loss of sensation on posterior thigh, leg, and plantar foot. Common Peroneal Nerve L4-S2 Trauma to lateral aspect of leg (e.g., fibular neck fracture), prolonged crossing of legs. Foot drop (loss of dorsiflexion), steppage gait. Loss of sensation on dorsum of foot/lateral shin. Tibial Nerve L4-S3 Deep laceration to popliteal fossa, tarsal tunnel syndrome. Loss of plantarflexion/foot inversion, toe flexion. Loss of sensation on sole of foot. Tarsal tunnel syndrome: sensory loss over sole with intrinsic foot muscle weakness (plantarflexion/inversion intact). Superior Gluteal Nerve L4-S1 Injections into superomedial buttock. Trendelenburg gait/sign (pelvis tilts to unaffected side when standing on affected leg). Inferior Gluteal Nerve L5-S2 Pelvic fracture, surgery. Weakness in hip extension (gluteus maximus). Difficulty climbing stairs, standing from seated position. Pudendal Nerve S2-S4 Stretch injury during childbirth, prolonged cycling. Perineal pain, fecal/urinary incontinence, sexual dysfunction. (Pudendal nerve block at ischial spine tip for anesthesia). Hip Muscles Action Major Muscles Flexors Iliopsoas, Sartorius, Tensor fascia lata, Pectineus. Extensors Gluteus maximus, Hamstrings (Semimembranosus, Semitendinosus, Biceps femoris). Abductors Gluteus medius, Gluteus minimus. Adductors Adductor magnus, longus, brevis. Internal Rotators Gluteus medius, Gluteus minimus, Tensor fascia lata. External Rotators Iliopsoas, Gluteus maximus, Piriformis, Obturator. Psoas Muscle: Origin T12-L5 vertebrae, insertion lesser trochanter. Hip flexion. Psoas Abscess: Fever, back/flank pain, inguinal mass, difficulty walking. Pain exacerbated by hip extension (psoas sign). Piriformis Syndrome: Muscle injury/hypertrophy compresses sciatic nerve. Sciatica-like symptoms. COMMON MUSCULOSKELETAL CONDITIONS Iliotibial Band Syndrome: Overuse injury in runners. Friction of IT band against lateral femoral epicondyle. Medial Tibial Stress Syndrome ("Shin Splints"): Overuse, bone resorption outpaces formation in tibial cortex. Limb Compartment Syndrome: ↑ Pressure in fascial compartment. Causes: Long bone fractures, reperfusion injury, animal venoms. 6 P's: Pain (out of proportion), Paresthesias, Pulselessness, Poikilothermia, Pallor, Paralysis. Motor deficits are late, irreversible. Surgical emergency. Plantar Fasciitis: Inflammation of plantar aponeurosis. Heel pain (worse with first steps in morning). De Quervain Tenosynovitis: Noninflammatory thickening of abductor pollicis longus & extensor pollicis brevis tendons. Pain/tenderness at radial styloid. ⊕ Finkelstein test. Ganglion Cyst: Fluid-filled swelling (herniation of dense connective tissue), most common at dorsal wrist. CHILDHOOD MUSCULOSKELETAL CONDITIONS Developmental Dysplasia of the Hip (DDH): Abnormal acetabulum development. Associated with "4 F's": Females, Firstborns, Fanny first (breech), Family history. Diagnosis (clinical): Barlow's (dislocate), Ortolani's (reduce), Galeazzi's (unequal knee heights), Trendelenburg sign (older patients). Confirmed by ultrasound. Treatment: Pavlik harness ( 15mo). Legg-Calvé-Perthes Disease: Idiopathic avascular necrosis of femoral head. 5-7 years old, insidious hip pain/limp. Slipped Capital Femoral Epiphysis (SCFE): Femoral head epiphysis displaces relative to femoral neck. Obese ~12-year-old with hip/knee pain and altered gait. Surgical treatment. Osgood-Schlatter Disease (Tibial Tubercle Apophysitis): Overuse injury of tibial tubercle. Repetitive quadriceps contraction $\rightarrow$ patellar tendon separates from tibial tubercle. Adolescents (12-15), running/jumping athletes. Progressive anterior knee pain, enlarged/tender tibial tubercle, pain on resisted knee extension. Radial Head Subluxation ("Nursemaid's Elbow"): Sudden pull on arm in children PHYSIOLOGY - Muscle Contraction Skeletal Muscle: Sarcomere: Functional unit. Distance between Z lines. Z Line: Anchors actin. Contains vimentin, desmin. I Band: Actin only. Shrinks with contraction. A Band: Myosin span. Constant length. H Zone: Myosin only (center of A band). Shrinks with contraction. M Line: Anchors myosin. Triad: 1 T-tubule + 2 terminal cisternae. Contraction Sequence: AP $\rightarrow$ ACh release $\rightarrow$ muscle cell depolarization. Depolarization travels via T-tubules. DHPR conformational change $\rightarrow$ opens ryanodine receptor (RR) on SR $\rightarrow$ Ca$^{2+}$ release. Ca$^{2+}$ binds Troponin C $\rightarrow$ shifts tropomyosin $\rightarrow$ exposes myosin-binding sites on actin. Myosin head binds actin, Pi released $\rightarrow$ power stroke (myosin pulls actin). H & I bands shorten, Z lines move closer. A band constant. ADP released. New ATP binds myosin $\rightarrow$ detachment from actin. ATP hydrolysis $\rightarrow$ myosin head re-cocked. Ca$^{2+}$ resequestered by SERCA. Types of Skeletal Muscle Fibers: Type 1 (Slow Twitch, Red): ↑ Mitochondria, myoglobin (oxidative phosphorylation). Resists fatigue. Sustained contraction (e.g., paraspinal muscles). "1 slow red ox." Type 2 (Fast Twitch, White): ↓ Mitochondria, myoglobin; ↑ glycogen (anaerobic glycolysis). Fast, powerful contractions (e.g., eye muscles). Malignant Hyperthermia: Dangerous reaction to anesthetics (halothane, succinylcholine). Abnormal ryanodine receptors $\rightarrow$ excessive Ca$^{2+}$ release $\rightarrow$ ATP consumption $\rightarrow$ heat, muscle rigidity. Treat with Dantrolene (RR antagonist). Cardiac Muscle: Striated, sarcomeres. Dyads: 1 T-tubule + 1 terminal cisternae. Ca$^{2+}$ influx via L-type Ca channels (DHPRs) triggers SR Ca$^{2+}$ release ("calcium-triggered calcium release"). Lusitropy (relaxation): Mediated by SERCA. Phospholamban (PLB) inhibits SERCA. Sympathetic stimulation $\rightarrow$ phosphorylates PLB $\rightarrow$ ↓ PLB $\rightarrow$ ↑ SERCA $\rightarrow$ faster relaxation/contraction. Smooth Muscle: Thick filament regulated (MLC phosphorylation). MLC phosphorylation by MLC kinase (MLCK) (activated by Ca$^{2+}$-calmodulin) $\rightarrow$ contraction. MLC phosphatase $\rightarrow$ relaxation. Contraction/tone regulated by intracellular Ca$^{2+}$ and MLC phosphorylation. ACh causes relaxation indirectly via endothelium (NO production). PHYSIOLOGY - Bone Formation & Remodeling Bone Matrix: Type I collagen + hydroxyapatite. Synthesized by osteoblasts as osteoid (non-mineralized). Endochondral Ossification: Cartilaginous model replaced by bone. Forms axial/appendicular skeleton, base of skull. Defective in achondroplasia. Membranous Ossification: Woven bone formed directly from mesenchymal tissue. Forms calvarium, facial bones, clavicle. Cells: Osteoblasts: Builds bone. Secrete collagen, catalyze mineralization (via ALP). Differentiate from mesenchymal stem cells. Markers: Bone ALP (creates alkaline media), Osteocalcin, Type I procollagen. Osteoclasts: Dissolves bone. Secrete H$^+$ and collagenases. Differentiate from monocyte/macrophage lineage. Stimulated by RANKL (from osteoblasts). Inhibited by Osteoprotegerin (OPG), which acts as decoy receptor for RANKL. Markers: Tartrate-resistant acid phosphatase, Urinary hydroxyproline, Urinary deoxypyridinoline (most reliable). Osteocytes: Inhabit lacunae. Sense mechanical stress, modulate osteoblast activity (sclerostin, FGF23). Maintain mineralized matrix, short-term Ca homeostasis. Bone Remodeling Key Substances: PTH: Low/intermittent levels $\rightarrow$ anabolic (bone building). Chronic ↑ levels $\rightarrow$ catabolic. PTH acts on osteoblasts, which then stimulate osteoclasts via RANKL, M-CSF and ↓ OPG. Estrogen: Inhibits osteoblast apoptosis, induces osteoclast apoptosis. Stimulates OPG synthesis. Causes epiphyseal plate closure. Deficiency $\rightarrow$ ↑ bone resorption, osteoporosis. Osteocalcin: From osteoblasts. Marker for bone remodeling. Sclerostin: Secreted by osteocytes. Inhibits osteoblastic bone deposition. FGF23: Secreted by osteocytes in response to hyperphosphatemia. Inhibits renal phosphate reabsorption, ↓ vitamin D synthesis. Unregulated secretion $\rightarrow$ hypophosphatemia, osteomalacia. Calcitonin: From parafollicular C-cells. Inhibits osteoclasts $\rightarrow$ ↓ bone resorption. Opposite of PTH. MSK PATHOLOGY Achondroplasia: Most common dwarfism. Activating mutation in FGFR3 $\rightarrow$ ↓ chondrocyte proliferation $\rightarrow$ ↓ endochondral ossification $\rightarrow$ short limbs. Autosomal dominant, ↑ paternal age. Membranous ossification unaffected (large head). Osteoporosis: Mass loss in trabecular (early) and cortical (late) bone. Normal mineralization and lab values (Ca$^{2+}$, PO4$^{3-}$, PTH). Causes: Primary (↓ estrogen, old age), Secondary (drugs, hyperparathyroidism, hyperthyroidism, multiple myeloma, malabsorption). Risk factors: Low peak bone mass (genetics, diet, exercise), rate of bone loss. Presentation: Low impact fractures (vertebral compression, hip, distal radial/Colles), acute back pain, loss of height, kyphosis. Diagnosis: DEXA scan (T-score $\le -2.5$). Glucocorticoids: ↑ Osteoclast activity, ↓ osteoblast activity, ↓ intestinal Ca$^{2+}$ absorption. PPIs: ↑ risk (insoluble Ca$^{2+}$ requires acidic environment). Thiazide diuretics: ↑ Ca$^{2+}$ reabsorption, ↑ BMD, ↓ fracture risk. Osteopetrosis ("Marble Bone Disease"): Defective osteoclasts $\rightarrow$ thickened, dense bones prone to fracture. Mutations (e.g., carbonic anhydrase II) impair acidic environment for resorption. Overgrowth fills marrow space $\rightarrow$ pancytopenia. Cranial nerve impingement. X-rays show diffuse sclerosis ("bone-in-bone"). Bone marrow transplant curative. Osteomalacia/Rickets: Defective mineralization of osteoid (osteomalacia) or growth plates (rickets). Most common cause: Vitamin D deficiency. X-rays: Osteopenia, "Looser zones" (pseudofractures) in osteomalacia. Epiphyseal widening, metaphyseal cupping/fraying in rickets. Rickets presentation: Bow legs (genu varum), rachitic rosary (bead-like costochondral junctions), craniotabes (soft skull), frontal bossing, pigeon breast. Labs: ↓ Vit D $\rightarrow$ ↓ Ca$^{2+}$ $\rightarrow$ ↑ PTH $\rightarrow$ ↓ PO4$^{3-}$. ↑ ALP. Paget Disease of Bone (Osteitis Deformans): Imbalance of osteoclast/osteoblast function. Pathogenesis: ↑ Osteoclastic activity (abnormally large, multinucleated) followed by ↑ osteoblastic activity forming poor quality bone. Stages: Lytic $\rightarrow$ Mixed $\rightarrow$ Sclerotic. End result: thickened, deformed, weaker bone. Histology: Mosaic pattern of woven/lamellar bone, cement lines. Presentation: Bone pain, ↑ hat size, hearing loss (auditory foramen narrowing), lion-like facies. Labs: Isolated ↑ ALP. Ca$^{2+}$, PO4$^{3-}$, PTH normal. Complications: High-output heart failure (AV shunts), ↑ risk of osteogenic sarcoma. Treatment: Bisphosphonates, calcitonin. Osteonecrosis (Avascular Necrosis): Infarction of bone/marrow. Most common site: femoral head (medial circumflex femoral artery insufficiency). Presentation: Pain on weight bearing, ↓ ROM. No swelling/erythema/warmth. Causes (CAST Bent LEGS): Corticosteroids, Alcoholism, Sickle cell, Trauma, The Bends, Legg-Calvé-Perthes, Gaucher, Slipped capital femoral epiphysis. Lab Values in Bone Disorders Condition Ca$^{2+}$ PO4$^{3-}$ ALP PTH Normal Normal Normal Normal Normal Osteoporosis Normal Normal Normal Normal Osteomalacia/Rickets ↓ ↓ ↑ ↑ Paget Disease Normal Normal ↑ Normal Primary Hyperparathyroidism ↑ ↓ ↑ ↑ Secondary Hyperparathyroidism ↓ ↑ ↑ ↑ Familial Hypocalciuric Hypercalcemia ↑ Normal Normal Normal Hypercalcemia of Malignancy ↑ ↓ Normal or ↑ ↓ Humoral Hypercalcemia of Malignancy (HHM): Hypercalcemia without focal lytic lesions. Caused by PTHrP secretion. More severe hypercalcemia than primary hyperparathyroidism. PRIMARY BONE TUMORS Tumor Type Epidemiology Location Characteristics Benign Tumors Osteochondroma Most common benign bone tumor. Males Metaphysis of long bones near growth plate. Cartilage-capped tumor with bony stalk, continuous with marrow space. Rarely transforms to chondrosarcoma. Osteoma Middle age. Surface of facial bones. Associated with Gardner syndrome. Osteoid Osteoma Adults females. Cortex of long bones (diaphysis). Benign osteoblast tumor with radiolucent osteoid core ( Osteoblastoma Vertebrae. Similar to osteoid osteoma but larger (>2cm), pain unresponsive to NSAIDs. Chondroma Medulla of small bones of hand/feet. Benign cartilage tumor. Giant Cell Tumor 20-40 years old. Epiphysis of long bones (often knee region). Locally aggressive. Neoplastic mononuclear cells (express RANKL) + reactive multinucleated giant cells. "Soap bubble" appearance on x-ray. Malignant Tumors Osteosarcoma 20% of 1° bone cancers. Peak Metaphysis of long bones (often knee region). Pleomorphic osteoid-producing cells. Painful enlarging mass, pathologic fractures. Codman triangle, sunburst pattern on x-ray. Aggressive. Chondrosarcoma Medulla of pelvis and central skeleton. Malignant chondrocytes. Ewing Sarcoma Caucasians, boys Diaphysis of long bones (femur), pelvic flat bones. Anaplastic small blue cells (neuroectodermal origin). t(11;22) (EWS-FLI1 fusion). "Onion skin" periosteal reaction. Aggressive, but responsive to chemotherapy. Bone Metastasis: More common than 1° bone tumors. Adults (>40): Prostate, breast, kidney, lung. Children: Neuroblastoma, Wilms Tumor, Osteosarcoma, Ewing Sarcoma, Rhabdomyosarcoma. Typically multifocal. Most involve axial skeleton or proximal femur. Fibrous Dysplasia: Benign tumor, components of normal bone but undifferentiated. Bone replaced by fibrous tissue. Somatic gain-of-function mutation of GNAS1 gene (constitutively active Gs protein). X-ray: "Bubbly lytic lesion" / "Ground glass." Histology: Curvilinear trabeculae ("Chinese characters"). Clinical patterns: Monostotic, Polyostotic, Mazabraud Syndrome (FD + soft tissue myxomas). McCune-Albright Syndrome (MAS): Triad: Polyostotic fibrous dysplasia (unilateral), Endocrine abnormalities (e.g., precocious puberty), Cafe-au-lait spots ("coast of Maine" border). RHEUMATOLOGY Osteoarthritis vs. Rheumatoid Arthritis Feature Osteoarthritis Rheumatoid Arthritis Pathogenesis Mechanical wear & tear destroys articular cartilage. Chondrocytes mediate degradation. Autoimmune inflammation of synovium $\rightarrow$ pannus formation (granulation tissue) $\rightarrow$ erodes cartilage/bone. Myofibroblasts $\rightarrow$ deformity. Predisposing Factors Age, female, obesity, joint trauma. Female, HLA-DR4, smoking. ⊕ RF, anti-CCP (more specific). Presentation Pain in weight-bearing joints after use, improves with rest. Asymmetric. No systemic symptoms. Pain, swelling, morning stiffness (>1hr), improves with use. Symmetric. Systemic symptoms (fever, fatigue, weight loss). Extraarticular manifestations common. Joint Findings Osteophytes (bone spurs), asymmetrical joint space narrowing, subchondral sclerosis/cysts. Synovial fluid noninflammatory (WBC Margin erosions, peri-articular osteopenia, soft tissue swelling, subchondral cysts, joint space narrowing. Deformities (cervical subluxation, ulnar deviation, swan neck, boutonniere). Synovial fluid inflammatory (WBC >2000). Affected Joints Large joints (knee, hip), DIP (Heberden nodes), PIP (Bouchard nodes), 1st carpometacarpal. Not MCP. Small joints (MCP, PIP, wrist). Not DIP or 1st CMC. Cervical spine involvement (subluxation, cord compression). Treatment Acetaminophen, NSAIDs, intra-articular glucocorticoids. NSAIDs, glucocorticoids, DMARDs (methotrexate, sulfasalazine, hydroxychloroquine, leflunomide), biologic agents (TNF-α inhibitors). Extraarticular Manifestations of RA: Rheumatoid nodules, Baker cyst, carpal tunnel, interstitial lung disease, pleuritis, anemia of chronic disease, Felty syndrome (neutropenia + splenomegaly), pericarditis, vasculitis, AA amyloidosis, Sjögren syndrome, scleritis. Seronegative Spondyloarthritis (PAIR) Arthritis without rheumatoid factor. Strong association with HLA-B27. Inflammatory back pain (morning stiffness, improves with exercise). Peripheral arthritis, enthesitis, dactylitis ("sausage fingers"), uveitis. Psoriatic Arthritis: Associated with skin psoriasis/nail lesions. Asymmetric, patchy. Dactylitis, "pencil-in-cup" deformity (DIP). Ankylosing Spondylitis: Symmetric involvement of spine/sacroiliac joints $\rightarrow$ "bamboo spine" (vertebral fusion). Males Extraskeletal: Restrictive lung disease, ascending aortitis (aortic insufficiency), anterior uveitis. Inflammatory Bowel Disease: Crohn's/UC associated with spondyloarthritis. Reactive Arthritis (Reiter Syndrome): "Can't see, can't pee, can't bend my knee" (Conjunctivitis, Urethritis, Arthritis). Preceding infection: Shigella, Yersinia, Chlamydia, Campylobacter, Salmonella (ShY ChiCS). Caused by immune complexes, joint aspirates are sterile. Cutaneous: Balanitis circinata, keratoderma blennorrhagicum. Crystal Arthropathies Gout: Acute inflammatory monoarthritis due to monosodium urate crystal precipitation. Crystals: Needle-shaped, ⊝ birefringent (yellow parallel, blue perpendicular). Risk factors: Male, hypertension, obesity, diabetes, dyslipidemia, hyperuricemia (underexcretion > overproduction). Alcohol, purine-rich foods, trauma. Presentation: Painful MTP joint of big toe (podagra). Tophus formation (chronic). Renal failure (urate nephropathy). Treatment: Acute (NSAIDs, glucocorticoids, colchicine). Chronic (allopurinol, febuxostat, probenecid, pegloticase). Calcium Pyrophosphate Deposition Disease ("Pseudogout"): Calcium pyrophosphate crystal deposition. Crystals: Rhomboid, weakly ⊕ birefringent (blue parallel). Etiology: Idiopathic, hemochromatosis, hyperparathyroidism, joint trauma. Presentation: >50 years. Pain/swelling with acute inflammation, chronic degeneration. Knee most common. Investigations: Chondrocalcinosis on x-ray. Treatment: Acute (NSAIDs, colchicine, glucocorticoids). Prophylaxis (colchicine). Other Connective Tissue Diseases Systemic Juvenile Idiopathic Arthritis: Most common arthritis in pediatric patients 2 joints). Leukocytosis, thrombocytosis, anemia, ↑ ESR/CRP. Sjögren Syndrome: Autoimmune destruction of exocrine glands (lacrimal, salivary). Mostly women 40-60. Primary or secondary (with RA, SLE, systemic sclerosis). Findings: Inflammatory joint pain, keratoconjunctivitis sicca (dry eyes), xerostomia (dry mouth), bilateral parotid enlargement. Investigations: ANA, RF. Anti-SSA (Ro), Anti-SSB (La). Lymphocytic sialadenitis on biopsy. Complications: Dental caries, MALT lymphoma. Septic Arthritis: S. aureus, Streptococcus, N. gonorrhoeae. Swollen, red, painful joint. Purulent synovial fluid (WBC >100,000), absent crystals. Gonococcal: purulent arthritis or triad of polyarthralgia, tenosynovitis, dermatitis. Systemic Lupus Erythematosus (SLE): Systemic autoimmune disease. Type III and Type II hypersensitivity. Associated with C1q, C4, C2 deficiency. Classic presentation: Rash, joint pain, fever in female of reproductive age. Libman-Sacks Endocarditis: Nonbacterial, verrucous thrombi (mitral/aortic valve, both surfaces). Lupus nephritis: Glomerular deposition of DNA-anti-DNA IC. Diffuse proliferative most common/severe. Causes of death: Renal disease, infections, cardiovascular disease. Drug-Induced Lupus Erythematosus (DILE): Lacks cutaneous/neurologic/renal manifestations. Rapid improvement on discontinuation. Procainamide, hydralazine, isoniazid (slow acetylators at higher risk). Antiphospholipid Syndrome: Primary or secondary (SLE). Clinical: Venous/arterial thromboembolic disease (DVT, PE, stroke), adverse pregnancy outcomes. Lab: Paradoxical aPTT prolongation (lupus anticoagulant effect), false positive VDRL/RPR. Anticardiolipin antibody, Beta-2 glycoprotein-1 antibody. Mixed Connective Tissue Disease: Features of SLE, systemic sclerosis, polymyositis. Associated with anti-U1 RNP antibodies. Polymyalgia Rheumatica: Pain/stiffness in proximal muscles (shoulders, hips). No weakness. Women >50. Associated with giant cell (temporal) arteritis. ↑ ESR, ↑ CRP, normal CK. Rapid response to low-dose corticosteroids. Fibromyalgia: Dysregulated neurotransmitter function $\rightarrow$ abnormal central processing of pain. Women 20-50. Treatment: Low-impact aerobic exercise, antidepressants (TCAs, SNRIs), anticonvulsants (Pregabalin, gabapentin). Avoid opioids/corticosteroids. Polymyositis / Dermatomyositis: Labs: ↑ CK, ⊕ ANA, ⊕ anti-Jo-1 (interstitial lung disease, nonerosive arthritis, "mechanic's hands"), ⊕ anti-SRP (prominent muscle weakness/atrophy), ⊕ anti-Mi-2 (Gottron papules, heliotrope rash). Associated with interstitial lung disease. Treatment: Steroids, immunosuppressants. Polymyositis: Progressive symmetric proximal muscle weakness. Endomysial inflammation, CD8+ T cells. Dermatomyositis: Similar to polymyositis + skin involvement. Malar rash, Gottron papules (violaceous papules over MCP/PIP/DIP), heliotrope rash (periorbital), "shawl and face" rash, "dirty" fingertips. ↑ risk of occult malignancy (gastric carcinoma). Perimysial/perifascicular inflammation, CD4+ T cells. X-linked Muscular Dystrophy: Muscle wasting, replacement by adipose tissue. Mutations in dystrophin (anchors cytoskeleton to ECM). Duchenne: Deletion of dystrophin. Proximal muscle weakness (1st year), calf pseudohypertrophy. ↑ CK. Death from cardiac/respiratory failure. Becker: Mutated dystrophin, milder disease. Neuromuscular Junction Diseases: Lambert-Eaton Myasthenic Syndrome: Autoantibodies to presynaptic Ca$^{2+}$ channels $\rightarrow$ ↓ ACh release. Proximal muscle weakness, eyes usually spared. Improves with muscle use. Associated with small cell lung cancer. Minimal effect with AChE inhibitors. Myasthenia Gravis: Autoantibodies to postsynaptic ACh receptor. Ptosis, diplopia, weakness (worsens with muscle use). Improves after edrophonium test. Associated with thymoma/thymic hyperplasia. Reverses with AChE inhibitors. Botulism: Blocks ACh release. Organophosphate Poisoning: Irreversibly inhibits AChE. Causes depolarizing paralysis. SLUDGE symptoms. Treat with Pralidoxime (if not "aged"), Atropine. Raynaud Phenomenon: Arteriolar vasospasm (cold/stress) $\rightarrow$ white $\rightarrow$ blue $\rightarrow$ red. Fingers/toes. Primary (idiopathic) or Secondary (mixed connective tissue disease, SLE, CREST). Digital ulceration in secondary. Treat with Ca$^{2+}$ channel blockers. Scleroderma (Systemic Sclerosis): Autoimmunity, noninflammatory vasculopathy, collagen deposition with fibrosis. Sclerosis of skin $\rightarrow$ puffy, taut skin, fingertip pitting. Can involve renal (crisis, treat with ACEi), pulmonary (interstitial fibrosis, HTN), GI (esophageal dysmotility/reflux), cardiovascular. Diffuse: Widespread skin, rapid progression, early visceral involvement. Anti-Scl-70 (anti-DNA topoisomerase I). Limited (CREST Syndrome): Limited skin (fingers, face). Calcinosis cutis, Raynaud, Esophageal dysmotility, Sclerodactyly, Telangiectasia. Anti-Centromere antibody. Pathologic Contractures: Congenital Torticollis: Dystonic sternocleidomastoid $\rightarrow$ head tilt. Birth trauma/intrauterine malposition. Volkmann's Ischemic Contracture: Muscle necrosis $\rightarrow$ irreversible contractures in forearm/wrist/hand. Compresses brachial artery/median nerve. Caused by supracondylar humerus fracture. Clubbing: Not fully elucidated. Associated with right-to-left shunts (cyanotic heart disease) $\rightarrow$ ↑ megakaryocytes/platelet clumps in peripheral circulation $\rightarrow$ release PDGF, VEGF $\rightarrow$ fibrovascular proliferation. ↑ PGE2 also implicated. DERMATOLOGY Skin Layers & Structures Epidermis (Ectoderm): Stratum corneum (keratin), lucidum, granulosum (granules), spinosum (desmosomes), basale (stem cells, regeneration, attached by hemidesmosomes). Dermis (Mesoderm): Subcutaneous fat (Hypodermis): Epithelial Cell Junctions: Tight Junctions (Zonula Occludens): Prevent paracellular movement. Adherens Junctions (Zonula Adherens): Actin filaments. Adhesion belt. Desmosomes (Macula Adherens): Intermediate filaments. Cell-to-cell adhesion. (Pemphigus Vulgaris targets desmoglein). Hemidesmosomes: Intermediate filaments. Cell-to-basement membrane adhesion. (Bullous Pemphigoid targets hemidesmosomes). Gap Junctions: Intercellular communication. Adnexal Components: Sweat Glands: Ducts open to skin surface. Myoepithelial cells. Sebaceous Glands: Associated with hair follicles. Produce sebum (holocrine). Stimulated by androgens. Dermatologic Macroscopic Terms Category >1 cm Flat Macule Patch Elevated Papule Plaque Fluid-filled Vesicle Bullae Pus-filled Pustule Petechiae ( 1cm): Red blood cell extravasation. Do not blanch. Telangiectasias: Small, focal, permanent dilatations of capillaries/venules. Blanch. Lentigo: Small tan/brown macule (sun-exposed). Melanocyte hyperplasia. Pigmented Skin Disorders Melanocytes: Basal layer, neural crest derived. Synthesize melanin in melanosomes (tyrosine precursor), pass to keratinocytes. Albinism: Congenital lack of pigmentation. Normal melanocyte number, ↓ melanin production due to ↓ tyrosinase activity or defective tyrosine transport. ↑ skin cancer risk. Vitiligo: Irregular patches of complete depigmentation. Autoimmune destruction of melanocytes. Associated with other autoimmune disorders. Melasma (Chloasma): Hyperpigmentation associated with pregnancy ("mask of pregnancy") or OCPs. Exacerbated by sun. Freckle (Ephelis): ↑ number of melanosomes (melanocytes not increased). Darken with sun. Pityriasis Versicolor (Tinea Versicolor): Hypo/hyperpigmented or erythematous macules/patches on upper body. Caused by Malassezia species (yeast). KOH prep: "spaghetti and meatballs" (spores & hyphae). Treat with topical antifungals, selenium shampoo. Nevus (Mole): Benign neoplasm of melanocytes. Congenital Nevus: Present at birth, often hairy. Acquired (Melanocytic) Nevus: Activating mutations (BRAF/NRAS). Intradermal: Melanocytes within dermis. Most common in adults. Junctional: Aggregates at dermoepidermal junction. Most common in children. Compound: Features of dermal and junctional. Dysplastic Nevus: Larger than acquired nevi, pigment variation, irregular borders. Possible melanoma precursor. Dysplastic Nevus Syndrome: Dozens/hundreds of nevi. Autosomal dominant, very high melanoma risk. Common Skin Disorders Seborrheic Dermatitis: Erythematous, well-demarcated plaques with greasy yellow scales in sebaceous-rich areas (scalp, face). Associated with Parkinson's, Malassezia. Acne: Chronic inflammation of hair follicles/sebaceous glands. Hormone-associated ↑ sebum (androgens). Keratin production blocks follicles $\rightarrow$ comedones. Cutibacterium acnes produces lipases $\rightarrow$ proinflammatory fatty acids. Comedones (blackheads/whiteheads), pustules, nodules. Drugs causing acne: Steroids, EGFR inhibitors, Lithium. Treatment: Retinoids (isotretinoin - teratogenic), benzoyl peroxide, antibiotics. Atopic Dermatitis (Eczema): Pruritic, erythematous, oozing rash with crusted lesions. Chronic course. Commonly on skin flexures (face in infancy, antecubital fossa in children/adults). Type I hypersensitivity. Associated with asthma, allergic rhinitis, food allergies. ↑ IgE, eosinophilia. Pathophysiology: Filaggrin gene mutations $\rightarrow$ barrier breakdown $\rightarrow$ dehydration, aeroallergen penetration. Allergic Contact Dermatitis: Pruritic, erythematous, oozing rash with vesicles/edema at site of contact (e.g., nickel, poison ivy, neomycin). Type IV hypersensitivity. Antigens presented by Langerhans cells to CD4+ T cells. Histology: Spongiosis (epidermal edema). Chronic: thickening of stratum spinosum/corneum. Pseudofolliculitis Barbae: "Razor bumps." Curly hair curls into skin $\rightarrow$ foreign body inflammatory reaction. Primarily African-American males. Psoriasis: Well-circumscribed, salmon-colored plaques with silvery scale. Extensor surfaces, scalp. Auspitz sign (pinpoint bleeding on scraping). Complications: Psoriatic arthritis, nail changes, uveitis. Pathophysiology: Excessive keratinocyte proliferation. Autoimmune (HLA-C). Biopsy: Acanthosis, parakeratosis, ↑ stratum spinosum, ↓ stratum granulosum. Neutrophils within epidermis (spongiform pustules), stratum corneum (Munro microabscesses). Elongation of dermal papillae. Treatment: Corticosteroids, PUVA, topical vitamin D analogs, immune-modulating therapy (cyclosporine, etanercept, methotrexate, ustekinumab). Rosacea: Inflammatory facial skin disorder. Erythematous papules/pustules (no comedones). Facial flushing. Rhinophyma (phymatous rosacea). Seborrheic Keratosis: Flat, greasy, pigmented squamous epithelial proliferation with keratin-filled cysts ("stuck on"). Common benign neoplasm of older persons. FGF23 activating mutations. Leser-Trélat sign: Sudden appearance of multiple seborrheic keratosis $\rightarrow$ underlying malignancy. Verrucae (Warts): HPV strains. Soft, tan, cauliflower-like papules. Epidermal hyperplasia, hyperkeratosis, koilocytosis. Urticaria (Hives): Pruritic wheals from mast cell degranulation. Histology: Superficial dermal edema. Skin Wrinkles (Aging): UVA $\rightarrow$ reactive oxygen species $\rightarrow$ ↓ collagen, ↑ MMPs $\rightarrow$ degrades collagen/elastin. Thinning epidermis, ↓ subcutaneous fat, flattened rete ridges. Vascular Tumors of Skin Angiosarcoma: Rare blood vessel malignancy (head, neck, breast, elderly, sun-exposed). Associated with radiation, chronic lymphedema, vinyl chloride/arsenic (hepatic). Aggressive. Bacillary Angiomatosis: Proliferation of blood vessels (capillary). Red-purple papules. AIDS patients, Bartonella infections (cat exposure). Neutrophilic infiltrate (vs. Kaposi sarcoma). Kaposi Sarcoma: Endothelial malignancy (skin, mouth, GI, respiratory). HHV-8, HIV. Lymphocytic infiltrate. Cherry Hemangioma (Senile Hemangioma): Small, bright-red papules. Most common benign vascular tumor in adults. Proliferation of capillaries/post-capillary venules in papillary dermis. Strawberry Hemangioma: Benign capillary hemangioma of infancy. Rapid growth, spontaneous regression. Cystic Hygroma: Lymphatic cysts. Posterior neck/lateral chest wall. Associated with Turner syndrome. Glomus Tumor: Benign, painful, red-blue tumor, commonly under fingernails. Arises from modified smooth muscle cells of thermoregulatory glomus body. Pyogenic Granuloma: Polypoid lobulated capillary hemangioma. Can ulcerate/bleed. Associated with trauma, pregnancy. Skin Infections Bacterial: Impetigo: Superficial. S. aureus or S. pyogenes. Honey-colored crusting. Bullous impetigo (S. aureus). Erysipelas: Upper dermis/superficial lymphatics. S. pyogenes. Well-defined, raised demarcation. Cellulitis: Dermal/subcutaneous. S. aureus or S. pyogenes. Red, tender, painful, swollen rash with fever. Can progress to necrotizing fasciitis. Abscess: Walled-off collection of pus. S. aureus. Necrotizing Fasciitis: Deeper tissue injury (anaerobic, S. pyogenes). Pain out of proportion. Crepitus. Bullae, purple skin. Surgical emergency. Staphylococcal Scalded Skin Syndrome (SSSS): Exotoxin destroys keratinocyte attachments in stratum granulosum. Fever, generalized erythematous rash with sloughing. ⊕ Nikolsky sign. Newborns, children, adults with renal insufficiency. Viral: Herpes: HSV-1/2. Herpes labialis, genitalis, herpetic whitlow. Molluscum Contagiosum: Umbilicated papules (poxvirus). Cytoplasmic inclusions (molluscum bodies). Varicella Zoster Virus: Varicella (chickenpox) - crops of lesions in various stages. Zoster (shingles) - dermatomal reactivation. Hairy Leukoplakia: Irregular, white, painless plaques on lateral tongue. EBV-mediated. HIV+, organ transplant recipients. Cannot be scraped off. Blistering Skin Disorders Pemphigus Vulgaris: Autoimmune destruction of desmosomes (IgG against desmoglein). Flaccid intraepidermal bullae of skin/oral mucosa. Acantholysis of stratum spinosum $\rightarrow$ suprabasal blisters. Basal layer attached ("tombstone"). Thin-walled bullae rupture easily (⊕ Nikolsky sign). Bullae spread laterally with pressure (Asboe-Hansen sign). Immunofluorescence: IgG surrounding keratinocytes ("fish net" pattern). Bullous Pemphigoid: Autoimmune destruction of hemidesmosomes (IgG against basement membrane collagen). Tense bullae of skin (oral mucosa spared). Basal cell layer detached from basement membrane. Tense bullae do not rupture easily (⊝ Nikolsky sign). Immunofluorescence: IgG along basement membrane (linear pattern). Dermatitis Herpetiformis: Autoimmune deposition of IgA at dermal papillae tips. Pruritic vesicles/bullae (grouped, herpetiform, elbows). Strong association with celiac disease. Resolves with gluten-free diet. Treatment: Dapsone. Erythema Multiforme (EM): Hypersensitivity reaction (cell-mediated, CD8+ T cells). Targetoid rash/bullae (central epidermal necrosis, erythema). Associated with HSV (most common), Mycoplasma, drugs (penicillin, sulfonamides), autoimmune, malignancy. EM with oral mucosa/fever $\rightarrow$ Stevens-Johnson Syndrome (SJS). Stevens-Johnson Syndrome (SJS): Fever, bullae, necrosis, sloughing of skin (dermal-epidermal junction). High mortality. Typically 2+ mucous membranes involved. Targetoid lesions. Usually adverse drug reaction. >30% BSA involved $\rightarrow$ Toxic Epidermal Necrolysis (TEN). 10-30% BSA $\rightarrow$ SJS-TEN. Miscellaneous Skin Disorders Acanthosis Nigricans: Epidermal hyperplasia $\rightarrow$ symmetric, hyperpigmented thickening (axilla, neck). Skin tags common. FGF23 activating mutations. Associated with insulin resistance (diabetes, obesity, Cushing), visceral malignancy (gastric adenocarcinoma). Actinic Keratosis: Premalignant lesions from sun exposure. Small, rough, erythematous papules with whitish scale. Risk of SCC proportional to dysplasia. Erythema Nodosum: Painful, raised inflammatory lesions of subcutaneous fat (panniculitis), usually anterior shins. Delayed hypersensitivity. Associated with sarcoidosis, coccidioidomycosis, histoplasmosis, TB, streptococcal infections, leprosy, IBD. Lichen Planus: "6 P's": Pruritic, Purple, Polygonal Planar Papules and Plaques. Mucosal involvement $\rightarrow$ Wickham striae. Sawtooth infiltrate of lymphocytes at dermal-epidermal junction. Associated with hepatitis C. Pityriasis Rosea: "Herald patch" (single, round-to-oval, pink, scaly patch with raised border). Followed by "Christmas tree" distribution of scaly erythematous plaques on trunk. Self-resolving. Sunburn: Acute cutaneous inflammatory reaction $\rightarrow$ DNA mutations, keratinocyte apoptosis. UVB dominant in sunburn, UVA in tanning/photoaging. ↑ skin cancer risk. Pyoderma Gangrenosum: Noninfectious, inflammatory, painful necrotic ulcers. Immune dysregulation. Associated with IBD, RA. Tender red pustules $\rightarrow$ sharply demarcated ulcer with raised, violaceous border. Burn Classification Type Depth Appearance First-degree Superficial, epidermis only. Painful, erythematous, blanching. Second-degree Partial-thickness, epidermis and dermis. Blistered. Painful, erythematous, blanching. Heals without scarring. Third-degree Full-thickness, epidermis, dermis, hypodermis. Painless, waxy/leathery, nonblanching. Scars. Keloid: Excessive collagen formation beyond wound borders. Raised, painful, pruritic nodules. Disorganized collagen. Familial tendency. Caused by excessive TGF-β. Hypertrophic Scar: Confined to wound origin. Parallel collagen. May regress. PHARMACOLOGY Arachidonic Acid Pathway Enzyme/Mediator Function Drug Target Phospholipase A2 Converts membrane phospholipids to arachidonic acid. ⊖ Glucocorticoids 5-Lipoxygenase Converts arachidonic acid to 5-HPETE. ⊖ Zileuton COX-1 Converts arachidonic acid to cyclic endoperoxides. ⊖ ASA, other NSAIDs (except celecoxib) COX-2 Converts arachidonic acid to cyclic endoperoxides (inflammatory cells, vascular endothelium). ⊖ Celecoxib Leukotrienes (LTC4, LTD4, LTE4) Bronchial tone. ⊖ Montelukast, Zafirlukast Leukotrienes (LTB4) Neutrophil chemotaxis. Prostacyclin (PGI2) Inhibits platelet aggregation, vasodilation. ⊕ Epoprostenol Prostaglandins (PGE1) Vascular tone (vasodilation), maintains PDA. ⊕ Alprostadil Prostaglandins (PGE2) Uterine tone (contraction), fever, pain. ⊕ Dinoprostone Prostaglandins (PGF2α) Uterine tone (contraction). ⊕ Carboprost Thromboxane (TXA2) Promotes platelet aggregation, vasoconstriction. Corticosteroids: Inhibit Phospholipase A2. Bind cytosolic glucocorticoid receptor, translocate to nucleus $\rightarrow$ altered gene expression. Acetaminophen: Reversibly inhibits COX (mostly CNS). Antipyretic, analgesic. Overdose $\rightarrow$ hepatic necrosis (NAPQI depletes glutathione). Antidote: N-acetylcysteine. Aspirin: Irreversibly inhibits COX-1/2 (covalent acetylation). ↓ TXA2, prostaglandins. ↑ bleeding time. Low dose: ↓ platelet aggregation. Intermediate: antipyretic, analgesic. High: anti-inflammatory. Adverse: Gastric ulceration/bleeding, tinnitus, allergic reactions, ↑ bleeding, Reye syndrome in children. Celecoxib: Reversibly, selectively inhibits COX-2. Spares COX-1 (gastric mucosa, platelet function). ↑ risk of thrombosis. Sulfa allergy. NSAIDs (Ibuprofen, naproxen, indomethacin): Reversibly inhibit COX-1/2. Block prostaglandin synthesis. Adverse: Interstitial nephritis, gastric ulcer, renal ischemia, aplastic anemia. Leflunomide: Reversibly inhibits dihydroorotate dehydrogenase (pyrimidine synthesis). Suppresses T-cell proliferation. RA, psoriatic arthritis. Teratogenic. Bone & Gout Drugs Bisphosphonates (Alendronate, Zoledronate): Pyrophosphate analogs. Bind hydroxyapatite, inhibit osteoclast activity, induce osteoclast apoptosis. ↓ bone loss, ↑ BMD. Uses: Osteoporosis, hypercalcemia, Paget disease. Adverse: Esophagitis, osteonecrosis of jaw, atypical femoral stress fractures. Teriparatide: Recombinant PTH analog. ↑ Osteoblastic activity (pulsatile). ↑ bone growth. Adverse: ↑ Osteosarcoma risk (avoid in Paget, history of cancer/radiation). Transient hypercalcemia. SERMs (Raloxifene): Estrogen actions on bone, anti-estrogen on breast/uterus. Uses: Osteoporosis, breast cancer prevention. Adverse: Hot flashes, DVT/PE. Gout Drugs: Acute: NSAIDs (indomethacin), Glucocorticoids, Colchicine (binds tubulin, impairs neutrophil chemotaxis/degranulation). Chronic (Preventive): Allopurinol: Competitive xanthine oxidase inhibitor. ↓ uric acid synthesis. Also for tumor lysis syndrome. ↑ azathioprine/6-MP levels. Febuxostat: Non-competitive xanthine oxidase inhibitor. Probenecid: Inhibits uric acid reabsorption in PCT. Can precipitate uric acid calculi. Pegloticase: Recombinant uricase (uric acid oxidase). Catalyzes uric acid to allantoin. PEGylated for prolonged half-life. Rasburicase: Recombinant uricase. Rapid on/off. Used in tumor lysis syndrome. DMARDs & Biologics TNF-α Inhibitors (Etanercept, Infliximab, Adalimumab): For RA, other autoimmune diseases. Etanercept: Fusion protein (soluble TNF-α receptor + Fc of IgG1). Decoy receptor. Methotrexate: First-line DMARD for moderate-severe RA. Folate antimetabolite $\rightarrow$ inhibits purine/pyrimidine synthesis (irreversible DHFR binding). Adverse: Oral/GI mucositis, alopecia, pancytopenia, hepatoxicity, pulmonary fibrosis, opportunistic infections.